
For years, researchers dismissed the brain’s background activity as useless noise. Now, the past researchers’ trash is the current researchers’ treasure.

The Brain by Matthew T. Ross
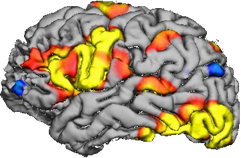
You have probably seen images of the brain illuminated with bursts of color. Hot reds and yellows representing higher levels of neural activity; cool blues and greens indicating relative calm. These activity patterns represent the brain’s responses to certain tasks at hand. If a scientist were to ask you to read this article aloud while lying in a brain scanner, you would see splotches of red around brain areas responsible for vision and language (similar to what is pictured below) on the corresponding scan. However, task-based responses account for a small portion of typical brain activity patterns. In fact, another kind of brain activity has garnered interest recently that could be used as a marker of normal brain functionality.
 |
| http://www.nedsahin.com/methods/fmri/ |
Prior to reading this article in the scanner, your brain would be in a resting state. This resting state may be found during introspective thought or daydreaming, but a resting state is not a quiet state. While resting, the brain is home to a constant hum of activity, like the static of an old television. It appears random, but in fact, this brain noise is due to slow and rhythmic signaling between groups of neurons in different brain regions. These coordinated groups are called neural networks. The brain shifts through different combinations of active brain regions so that many possible neural network configurations can arise over time. And the ability to shift configurations may play a huge role in brain health.
Computer models of neural networks indicate noise allows the brain to "explore" different areas of parameter space, or its dynamic range, by jumping between different neural network configurations. To go between these configurations, different brain regions rapidly and randomly jump between peaks and valleys of activity states. A combination of bursting and silence across different groups of brain regions at one point in time converges into a brief, stable network configuration, ready to collapse into a new configuration with a slight nudge. By operating at the border of chaos and stability, the brain enters a state of anticipation that expands the range of inputs it can process and balances that input range with the amount of information it can output (Ghosh et al, 2008). This was elegantly described by Gustavo Deco and colleagues:
A recent study published in the Journal of Neuroscience shows how changing the brain’s noise levels can be pathological (Mišić et al, 2016). Posttraumatic stress disorder (PTSD) includes well-known psychological symptoms of persistent negative feelings and recurring intrusive flashbacks related to a traumatic experience. The present study by Bratislav Mišić and colleagues joins a growing body of experimental evidence underlying the neurophysiological characteristics of PTSD, thus identifying a clinically relevant biomarker for PTSD diagnosis.
The neural correlate Mišić and colleagues found turned out to be a lack of brain noise. The researchers scanned the brains of military veterans with PTSD compared to the following controls: veterans without PTSD, civilians, and civilians with traumatic brain injury (commonly concomitant with PTSD in veterans). Intriguingly, only the veterans with PTSD exhibited “hypersynchrony” between key brain regions involved in emotions and memory, including the hippocampus, amygdala, and posterior cingulate cortex. In this way, the variability of activity within the resting neural network, or its noisiness, was reduced.
Computer models of neural networks indicate noise allows the brain to "explore" different areas of parameter space, or its dynamic range, by jumping between different neural network configurations. To go between these configurations, different brain regions rapidly and randomly jump between peaks and valleys of activity states. A combination of bursting and silence across different groups of brain regions at one point in time converges into a brief, stable network configuration, ready to collapse into a new configuration with a slight nudge. By operating at the border of chaos and stability, the brain enters a state of anticipation that expands the range of inputs it can process and balances that input range with the amount of information it can output (Ghosh et al, 2008). This was elegantly described by Gustavo Deco and colleagues:
"Metaphorically speaking, the resting state is like a tennis player waiting for the service of his opponent. The player is not statically at rest, but rather actively moving making small jumps to the left and to the right, because in this way, when the fast ball is coming, he can rapidly react."Our tennis player must balance the probability of receiving the serve (the input range) and whacking the ball with as much force as he can muster (the output level). At a certain range of jitter, our tennis player, like the brain at rest, maximizes both his dynamic range and the power of his output.
A recent study published in the Journal of Neuroscience shows how changing the brain’s noise levels can be pathological (Mišić et al, 2016). Posttraumatic stress disorder (PTSD) includes well-known psychological symptoms of persistent negative feelings and recurring intrusive flashbacks related to a traumatic experience. The present study by Bratislav Mišić and colleagues joins a growing body of experimental evidence underlying the neurophysiological characteristics of PTSD, thus identifying a clinically relevant biomarker for PTSD diagnosis.
The neural correlate Mišić and colleagues found turned out to be a lack of brain noise. The researchers scanned the brains of military veterans with PTSD compared to the following controls: veterans without PTSD, civilians, and civilians with traumatic brain injury (commonly concomitant with PTSD in veterans). Intriguingly, only the veterans with PTSD exhibited “hypersynchrony” between key brain regions involved in emotions and memory, including the hippocampus, amygdala, and posterior cingulate cortex. In this way, the variability of activity within the resting neural network, or its noisiness, was reduced.
 |
Diffusion tensor imaging showing connectivity between brain regions. By Alfred Anwander, Wikimedia Creative Commons |
{kind=link}
A lack of noise is associated with disorder, but what about too much noise? In theory, a high level of noise can swallow up important signals. Recall those colored brain scan images. If the background noise in a brain area is initially high, then when that area “lights up” during a task it will be masked by the noise and appear inactive. It turns out that large levels of noise in the brain correlate with psychosis. When people consume the active component in cannabis called THC, background activity in the brain increases (Cortes-Briones et al, 2015). With high doses of THC that produce "psychosis-like effects," the resting brain activity of people, as measured by electroencephalography (EEG), is noisier than if they are given a placebo.
Clearly, the brain needs a certain level of noise to maintain normal functioning, but why does noise matter so much? The brains of the veterans with PTSD in the above study seem to be stuck in a rut of parameter space. They may be unable to break free because the lack of variability has trapped brain networks into a single, stable configuration centered around their traumatic memories. In our tennis example, it seems that when the serve comes barreling over the net, the veterans with PTSD react as though they have bricks in their pockets. Perhaps these patients’ brains are simply unable to think of things besides their traumatic memories.
Could we optimize the brain's noise levels and return the dynamic range back to normal? This is a complex question. For one, we don't know whether noise decreases as a result of PTSD or whether abnormal brain noise predisposes a person to develop PTSD. While the imaging and EEG studies mentioned earlier provide us with a correlation between cognition and the brain's state of affairs, we have no access to the brain's history prior to the noise change and can only speculate about what may have been the trigger. Yet, studies like the one with THC show us that drugs can dramatically affect the brain's background noise level. If low noise levels are a cause of PTSD symptoms, perhaps THC could be used to increase noise levels in PTSD patients to appropriate levels.
In fact, a couple of studies looked into this very idea and found somewhat promising results. In 2014, a pilot study of orally administered THC found reduced severity of PTSD symptoms in most participants (Roitman et al, 2014). And last year, nabilone, a synthetic chemical that binds to the same class of cellular receptors as THC called "cannabinoid receptors," reduced the severity of nightmares experienced by the subjects with PTSD (Jetly et al, 2015).
Let's not get carried away, though. While this early research provides a glimmer of hope, there are many caveats. THC may alleviate symptoms, but it may not be directly through noise changes. And, even if cannabinoid treatment alleviated symptoms by changing brain noise, the lack of brain noise in patients with PTSD is probably not confined only to dysfunctional cannabinoid receptors. Since the brain's dynamic range is constrained in specific neural networks in PTSD, rescuing these networks could be at the expense of increasing noise in other networks, causing some other psychotic distress with long-term treatment. Attempting to fix one part of the brain with a treatment that targets the entire brain has been a continual struggle for modern medicine. Think of the seemingly never-ending list of side effects in commercials for anti-depressants.
Deep brain stimulation (DBS), a treatment that has seen a great deal of success in alleviating symptoms of Parkinson's disease, could be one alternative. In DBS, a thin wire is implanted into the brain to deliver mild shocks to brain cells. Exactly how this stimulation changes neuronal activity in a way that reduces symptoms remains a matter of debate. However, the effects of DBS are robust and clinicians are starting to apply DBS to treating a multitude of other brain diseases.
Perhaps with a better understanding of synchronized neural activity and how it plays into large network rhythmic activity, we could use DBS to reinstate the normal rhythms in the hypersynced brain networks of people with PTSD. In fact, a study found alleviation of PTSD-like symptoms in rats following DBS of the amygdala (Langevin et al, 2010), a region of the brain that is involved in emotion processing and part of the hypersynced network studied by Mišić and colleagues. Now, an ongoing 24-month Phase I trial of six veterans with severe PTSD is using DBS of the amygdala and has so far seen encouraging results of significantly decreasing symptom severity (Langevin et al, 2015).
These exciting studies and clinical trials are leading to a greater understanding of the brain’s dynamic states and how we can manipulate them to rescue dysfunctional networks. Perhaps soon we will rejoice in the clamor of patients’ noisy (and healthy) brains.
Clearly, the brain needs a certain level of noise to maintain normal functioning, but why does noise matter so much? The brains of the veterans with PTSD in the above study seem to be stuck in a rut of parameter space. They may be unable to break free because the lack of variability has trapped brain networks into a single, stable configuration centered around their traumatic memories. In our tennis example, it seems that when the serve comes barreling over the net, the veterans with PTSD react as though they have bricks in their pockets. Perhaps these patients’ brains are simply unable to think of things besides their traumatic memories.
Could we optimize the brain's noise levels and return the dynamic range back to normal? This is a complex question. For one, we don't know whether noise decreases as a result of PTSD or whether abnormal brain noise predisposes a person to develop PTSD. While the imaging and EEG studies mentioned earlier provide us with a correlation between cognition and the brain's state of affairs, we have no access to the brain's history prior to the noise change and can only speculate about what may have been the trigger. Yet, studies like the one with THC show us that drugs can dramatically affect the brain's background noise level. If low noise levels are a cause of PTSD symptoms, perhaps THC could be used to increase noise levels in PTSD patients to appropriate levels.
In fact, a couple of studies looked into this very idea and found somewhat promising results. In 2014, a pilot study of orally administered THC found reduced severity of PTSD symptoms in most participants (Roitman et al, 2014). And last year, nabilone, a synthetic chemical that binds to the same class of cellular receptors as THC called "cannabinoid receptors," reduced the severity of nightmares experienced by the subjects with PTSD (Jetly et al, 2015).
Let's not get carried away, though. While this early research provides a glimmer of hope, there are many caveats. THC may alleviate symptoms, but it may not be directly through noise changes. And, even if cannabinoid treatment alleviated symptoms by changing brain noise, the lack of brain noise in patients with PTSD is probably not confined only to dysfunctional cannabinoid receptors. Since the brain's dynamic range is constrained in specific neural networks in PTSD, rescuing these networks could be at the expense of increasing noise in other networks, causing some other psychotic distress with long-term treatment. Attempting to fix one part of the brain with a treatment that targets the entire brain has been a continual struggle for modern medicine. Think of the seemingly never-ending list of side effects in commercials for anti-depressants.
Deep brain stimulation (DBS), a treatment that has seen a great deal of success in alleviating symptoms of Parkinson's disease, could be one alternative. In DBS, a thin wire is implanted into the brain to deliver mild shocks to brain cells. Exactly how this stimulation changes neuronal activity in a way that reduces symptoms remains a matter of debate. However, the effects of DBS are robust and clinicians are starting to apply DBS to treating a multitude of other brain diseases.
Perhaps with a better understanding of synchronized neural activity and how it plays into large network rhythmic activity, we could use DBS to reinstate the normal rhythms in the hypersynced brain networks of people with PTSD. In fact, a study found alleviation of PTSD-like symptoms in rats following DBS of the amygdala (Langevin et al, 2010), a region of the brain that is involved in emotion processing and part of the hypersynced network studied by Mišić and colleagues. Now, an ongoing 24-month Phase I trial of six veterans with severe PTSD is using DBS of the amygdala and has so far seen encouraging results of significantly decreasing symptom severity (Langevin et al, 2015).
These exciting studies and clinical trials are leading to a greater understanding of the brain’s dynamic states and how we can manipulate them to rescue dysfunctional networks. Perhaps soon we will rejoice in the clamor of patients’ noisy (and healthy) brains.
References:
Cortes-Briones JA, Cahill JD, Skosnik PD, Mathalon DH, Williams A, Sewell RA, Roach BJ, Ford JM, Ranganathan M, D’Souza DC (2015) The Psychosis-like Effects of Δ(9)-Tetrahydrocannabinol Are Associated With Increased Cortical Noise in Healthy Humans. Biol Psychiatry 78:805–813.
Deco G, Jirsa V, McIntosh AR, Sporns O, Kötter R (2009) Key role of coupling, delay, and noise in resting brain fluctuations. Proceedings of the National Academy of Sciences 106:10302–10307.
Ghosh A, Rho Y, McIntosh AR, Kötter R, Jirsa VK (2008) Noise during rest enables the exploration of the brain’s dynamic repertoire. PLoS Comput Biol 4:e1000196.
Jetly R, Heber A, Fraser G, Boisvert D (2015) The efficacy of nabilone, a synthetic cannabinoid, in the treatment of PTSD-associated nightmares: A preliminary randomized, double-blind, placebo-controlled cross-over design study. Psychoneuroendocrinology 51:585–588.
Langevin J-PP, De Salles AA, Kosoyan HP, Krahl SE (2010) Deep brain stimulation of the amygdala alleviates post-traumatic stress disorder symptoms in a rat model. J Psychiatr Res 44:1241–1245.
Langevin J-PP, Koek RJ, Schwartz HN, Chen JW, Sultzer DL, Mandelkern MA, Kulick AD, Krahl SE (2015) Deep Brain Stimulation of the Basolateral Amygdala for Treatment-Refractory Posttraumatic Stress Disorder. Biol Psychiatry.
Mišić B, Dunkley BT, Sedge PA, Da Costa L, Fatima Z, Berman MG, Doesburg SM, McIntosh AR, Grodecki R, Jetly R, Pang EW, Taylor MJ (2016) Post-Traumatic Stress Constrains the Dynamic Repertoire of Neural Activity. J Neurosci 36:419–431.
Roitman P, Mechoulam R, Cooper-Kazaz R, Shalev A (2014) Preliminary, open-label, pilot study of add-on oral Δ9-tetrahydrocannabinol in chronic post-traumatic stress disorder. Clin Drug Investig 34:587–591.